Innovative modern diagnostic and imaging technologies developed over the past two decades have improved optometrists’ ability to detect eye diseases early and manage them effectively.

Unfortunately, group vision care plans have not kept pace with these innovations resulting in gaps in care. This means that eye diseases may be undetected in the early stages.
Diseases like glaucoma, diabetic retinopathy, and age-related macular degeneration (AMD) usually develop after age 40 and can have serious workplace consequences if they go undetected and untreated.
By providing a vision care benefit that includes modern diagnostics and imaging, plan sponsors can differentiate themselves in the competition for talent and address one of the highest levels of importance but the lowest levels of satisfaction in employee benefits.
The Canadian Association of Optometrists (CAO) calls upon group benefit stakeholders to modernize vision care benefits and fill the gaps in care by including a reasonable allowance for modern diagnostics and imaging procedures to help detect eye disease early and preserve the vision of working Canadians.
Early Detection and Disease Prevention
Chronic disease accounts for 65% of all Canadian deathsi and more than $190 billion in annual healthcare costs. ii Prevention, early detection, and treatment of chronic diseases, including those of the eye, is a cost-effective approach to effective disease management and preventing co-morbidities that can be life-changing or life-threatening. This handbook provides compelling evidence for adding an allowance for medically necessary modern diagnostics and imaging during comprehensive examinations and for follow-up testing when clinically indicated.
Several eye diseases are chronic ones that benefit from early detection and treatment, especially glaucoma, age-related macular degeneration (AMD), and diabetic and hypertensive retinopathy.
Early detection with screening is the best approach to preventing severe conditions and high treatment costs.
The Comprehensive Exam
Prevention Starts Here
A comprehensive eye examination is the best tool for the early detection of eye disease and several systemic diseases. It is based on the premise that structural change in the eye (often at the microscopic level) manifests itself well before any functional changes and vision loss occur (See Figure 1).
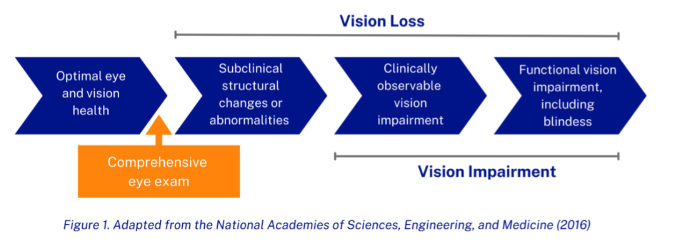
If performed according to recommended frequency guidelines, including diagnostic and imaging tools, more than 90% of vision loss in Canada can be detected early and prevented from progressing to functional vision impairment.iii
Today’s comprehensive eye examination has evolved and is not the same as in the 1970s, 1980s, and 1990s. The modern exam is anchored in the many technological and clinical advances of the 21st century. These modern diagnostic technologies are essential for detecting microscopic structural changes in the eye at the earliest signs of disease. They allow optometrists to not only detect eye disease but many other health conditions, including hypertension, cardiovascular disease, multiple sclerosis, tumors, Crohn’s Disease, and many others. iv
20% of Canadians have an eye disease that may lead to blindness.v
Many are in today's workforce.
Without early detection and treatment, the costs incurred by plan sponsors and insurers will be much higher in the long term when the diagnosis is delayed until the disease is symptomatic and has progressed to significant vision impairment.
Additional costs because of a delayed diagnosis will include prescription drugs, including treatment related to depression, injury, falls, nursing care, presenteeism, absenteeism, and disability.
The cost of early detection and management through modern diagnostics is not prohibitive. Although fees will vary by province, locality, and provider, the range for modern diagnostics and imaging is usually between $50 and $120 per test. For the average vision care plan, this is equivalent to less than one average- priced prescription drug claim per adult member every two years, if every plan member visits their optometrist every 24 months and is identified for diagnostics and imaging.
When patients do receive the necessary diagnostics and imaging during their comprehensive exam, if they have abnormal test results or are diagnosed with an eye disease, their optometrist will likely book a follow-up appointment sooner than 24 months. The cost for follow-up tests is in the same $50-$120 range per test. Follow-ups typically occur once or twice a year.
Components of the Comprehensive Eye Examination and Follow-Up Appointments
A comprehensive eye examination conducted by an optometrist is recommended once every 24 months for most adults and annually for most children and seniors.
The exam has 9 essential components:
- Medical and ocular history check
- Visual acuity examination and refraction
- Ocular motility examination
- Slit lamp examination of the anterior segment of the eye
- Visual field test by confrontation
- Fundus examination - dilated (when clinically indicated)
- Tonometry – measures intraocular pressure (when clinically indicated)
- Advice and instruction to the patient as needed
- Prescription and referral if indicated.
When age, personal or family medical history, or other factors indicate risk of disease, the eye exam would normally include one or more of the modern diagnostics and imaging tests listed on page 5. With these tools, the comprehensive eye examination becomes one of the best and most cost-effective preventive screening and diagnostic tools available.
Health Care Spending Accounts
Although some plan members may be encouraged to use their health care spending account (HCSA) to cover vision care expenses, a host of uninsured services are competing for these same dollars. Optometrists report that many plan members opt not to receive essential services either because they do not understand their value or because they cannot afford them.
Modern Diagnostics and Imaging Tools
Optical Coherence Tomography (OCT)
An imaging technique that uses light waves to create detailed 3D images of the layers of the retina. It is used to help diagnose and monitor the progression of eye diseases, including diabetic retinopathy, AMD, and glaucoma.
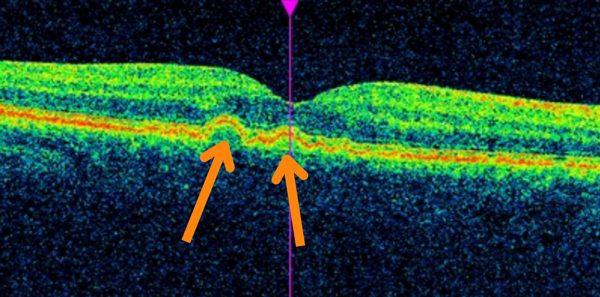
OCT with AMD
Heidelberg Retinal Tomography (HRT)
Similar to an OCT, the HRT is an imaging technique that uses a laser to create a 3D image of the back of the eye, particularly the optic nerve and retina. The purpose is to detect and monitor conditions that affect the optic nerve, such as glaucoma.
Full Threshold Visual Field Testing
This checks for any areas of vision loss or damage to the peripheral vision, which can be an early sign of eye diseases like glaucoma or retinal detachment. A special machine emits flashes of light to create a detailed map of an individual’s peripheral vision.
Retinal Imaging & Widefield Retinal Imaging
Retinal imaging is a medical imaging technique that allows optometrists to take images of the retina.
Widefield retinal imaging captures a wider area of the back of the eye than traditional imaging methods.
These images can help optometrists detect and monitor eye diseases, such as diabetic retinopathy, AMD, and glaucoma.
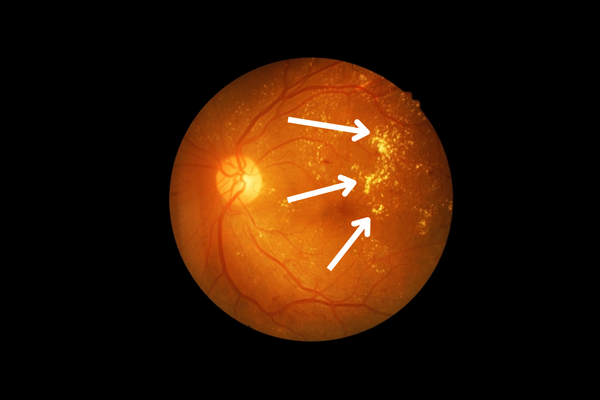
Retinal Image of Retinopathy
Autofluorescence
A special camera is used to capture images of the retina as it emits fluorescent light.
Images can provide information about any abnormalities or damage to the retina and detect a variety of eye diseases, including AMD.
Anterior Segment Photo Documentation
A medical imaging technique that captures detailed images of the front part of the eye, including the cornea, iris, and lens from different angles and positions. This helps optometrists diagnose and monitor eye conditions that affect the front part of the eye, including cataracts, glaucoma, and corneal disorders.
How Eye Disease Affects Working-Age Canadians
Eye disease including diabetic and hypertensive retinopathy, AMD, and glaucoma are all leading causes of vision loss that can affect individuals in their working years, particularly as we age.
Diabetic Retinopathy: Diabetic retinopathy affects approximately one million Canadiansv and manifests as dark patches of vision loss, which increase as the disease progresses. Unaddressed, diabetic retinopathy leads to retinal detachment and blindness. The odds of a person being unable to work because of diabetic retinopathy are roughly twice those of someone whose diabetes and retinopathy are under control. They are likely to have 40% more sick days.vi Benefit costs can reach almost $20,000 annually, nearly double of an employee with diabetes whose vision health is preserved.vi
Age-related Macular Degeneration (AMD): AMD affects approximately 2.5 million Canadiansvand manifests as a reduction of central vision, which increases as the disease progresses. There are AMD treatments that are successful in slowing down or stopping the progression of damage to the eye, thus preventing severe vision loss and additional costs to plan sponsors. However, optimal patient outcomes depend on early detection and consequent early treatment.vii
Glaucoma: Glaucoma affects nearly 750,000 Canadiansv and manifests as a reduction in peripheral vision. By the time a patient notices it, it is usually too late to prevent permanent vision loss. Peripheral vision continues to reduce as the disease progresses. Early detection of glaucoma is crucial to its successful management. In addition to the visual manifestations, one in five glaucoma patients suffer anxiety and depression, and 50% suffer sleep disorders. viii

Vision with Diabetic Retinopathy

Vision with AMD

Vision with Glaucoma
The Impact of Eye Disease on Quality of Life
If not caught early and stopped from progressing, eye disease will have a major
impact on a patient’s quality of life. The impact can be as severe as that of cardiovascular disease, kidney disease, and some cancers.
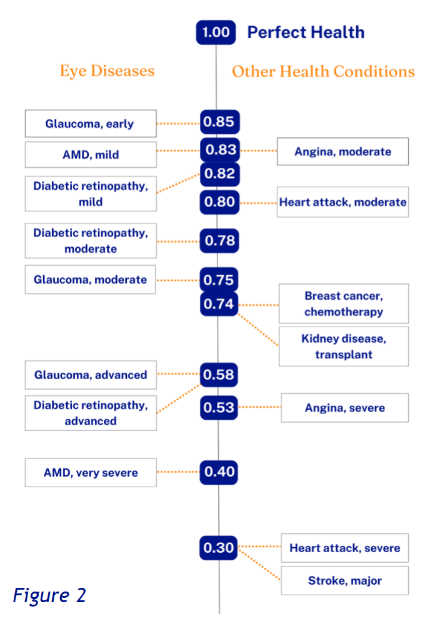
Figure 2 provides a numeric representation of the impact of eye disease on quality of life. It offers a comparison between some eye conditions and cardiovascular disease, kidney disease, and breast cancer.
Provincial Coverage
Provincial health plans do not cover vision care for working-age Canadians. This makes group vision care plans critically important for the maintenance of the vision health of working Canadians.
Some exceptions exist for those with a diagnosed eye disease. Comprehensive eye examination coverage is provided to children in some provinces, often with stringent age parameters. Patients with glaucoma, AMD, and diabetic retinopathy usually have access to some public coverage once the condition is at an advanced stage. For a working Canadian with group benefits, this would be too late to prevent permanent vision loss.
Closing the Gaps in Vision Care Coverage
Gaps in group vision care plans have developed as new clinical standards of practice and supporting technologies have become available, while group vision care coverage has not changed.
Filling the gaps in vision care benefits will not overburden group benefit plans. Just the opposite. Including coverage to identify and treat serious eye diseases early mitigates their debilitating and costly impact on plan sponsors when they are left undetected.
Current best practice vision care includes modern diagnostics and imaging when recommended by an optometrist during a comprehensive examination.
A small percentage of patients, usually in the 40 years or older age group, will require follow-up appointments to monitor their eyes for changes and signs of disease progression or, following a diagnosis of eye disease, to monitor the effectiveness of treatment and manage their condition.
Why expand coverage to include an allowance for diagnostics and imaging?
1 in 4 Canadians who have access to vision care benefits report not receiving services they need due to cost.
Abacus 2020
For the insurer and the plan sponsor who do not invest in prevention, unmanaged or advanced stages of disease can affect their benefits budget significantly and their bottom line. There is a significant burden because of the costs of drugs, absenteeism, presenteeism, and long- term disability associated with advanced stages of eye disease.
Working Canadians rely on their group vision care plans for their vision health, and they place a high value on the benefit. Plan sponsors who wish to attract talent should fill the gap in their vision care benefit by providing a benefit that includes modern diagnostics and imaging.
The Canadian Association of Optometrists calls upon group benefit stakeholders to review and modernize group vision care plan provisions, so they meet modern clinical standards of practice and the technological innovations that enable them.
To find out more, visit www.dontlosesight.ca
Follow the Canadian Association of Optometrists on LinkedIn
Contact us at dontlosesight@opto.ca or info@opto.ca
References
i. Statistics Canada. (2022). Table 13-10-0394-01: Leading causes of death, total population, by age group, 2019. Available from: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1310039401
ii. Elmslie, K. (2016). Against the growing burden of disease. Public Health Agency of Canada. Available from: https://cagh-acsm.org/sites/default/files/resources/2016/10/elmslie.pdf
iii. Steinmetz, J. D., Flaxman, S., Briant, P. S., Taylor, H. R., Resni
koff, S., ... & Tareque, M. I. (2021). Trends in prevalence of blindness and distance and near vision impairment over 30 years: an analysis for the Global Burden of Disease Study. The Lancet Global Health, 9(2), e130-e143. Available from: https://www.thelancet.com/journals/langlo/article/PIIS2214- 109X(20)30488-5/fulltext
iv. UnitedHealthcare. (2013). Integrating eye care with disease management: it's not just about diabetes anymore. Available from: https://www.unitedhealthgroup.com/content/dam/UHG/PDF/2013/UHCEyeCareDiseaseManagement.pdf
v. Deloitte. (2021, May). The cost of vision loss and blindness in Canada. Canadian Council of the Blind. Available from: https://www.fightingblindness.ca/wp-content/uploads/2021/12/Deloitte-Cost-of-vision- loss-and-blindness-in-Canada-report-May-2021.pdf
vi. Brook, R. A., Kleinman, N. L., Patel, S., Smeeding, J. E., Beren, I. A., & Turpcu, A. (2015). United States comparative costs and absenteeism of diabetic ophthalmic conditions. Postgraduate Medicine, 127(5), 455- 462. Available from: https://www.tandfonline.com/doi/abs/10.1080/00325481.2014.994468? journalCode=ipgm20
vii. Liu, L., & Swanson, M. (2013). Improving patient outcomes: role of the primary care optometrist in the early diagnosis and management of age-related macular degeneration. Clinical Optometry, 5, 1-12. Available from: https://www.dovepress.com/getfile.php?fileID=15245
viii. Groff, M. L., Choi, B., Lin, T., Mcllraith, I., Hutnik, C., & Malvankar, M. (2022). Anxiety, depression, and sleep-related outcomes of glaucoma patients: a systematic review and meta-analysis. Canadian Journal of Ophthalmology. Available from: https://www.sciencedirect.com/science/article/abs/pii/S0008418222000552


