Canada's first generic GLP-1 drugs are here – but plan sponsors shouldn't assume savings will arrive automatically, say experts
In the span of just three days, Canada became the first G7 country to approve not one but two generic versions of semaglutide – the active ingredient in Ozempic. Health Canada authorized a submission from India's Dr. Reddy's Laboratories on April 28, followed by a second from Toronto-based Apotex on May 1.
Seven more submissions are currently under review, with regulatory decisions expected in the coming weeks and months, according to Health Canada.
The milestone has drawn attention from HR and benefits professionals who have watched GLP-1 drug costs balloon over the past several years. But experts caution that the path from approval to real-world savings is more complicated than it appears.
A structural shift, not just a price drop
Helen Stevenson, founder and CEO of Reformulary Group and a former assistant deputy minister of health for Ontario, says the approvals are welcome news – but HR leaders need to understand how their plans are set up before expecting a big drop in drug benefit plan costs.
“We’re thrilled about it because, typically speaking, when a generic comes on the market, the price drops quite significantly – although how much really depends on how many generic versions of the drug there are,” she says. “Having two generics approved, I would speculate the price will be down to 50 per cent of the brand cost of Ozempic.”
Under Canada's pan-Canadian Pharmaceutical Alliance pricing structure, prices would fall further still if more generics reach the market – potentially to around 35 per cent of the brand-name price when three or more alternatives are available.
Brand-name Ozempic costs between $200 to $450 per month in Canada, with annual costs of more than $5,000 in some cases, according to integrated health-care platform Felix.
Generic substitution of Ozempic not automatic
The catch, says Stevenson, is that many employers moved Ozempic onto special authorization years ago, when off-label use for weight loss caused plan costs to skyrocket. Under special authorization, generic substitution doesn’t happen automatically.
“If [a drug plan] has had Ozempic requiring special authorization, they'll probably need to make a conscious decision to require that people use the generic versus the brand,” she says. “Plans are not going to uniformly see this sort of immediate benefit of lower cost.”
Her advice to HR and benefits leaders is to start by understanding exactly how Ozempic is currently reimbursed in their plan. Is it an open benefit where generic substitution is automatic, or does it require special approval? The answer determines what action, if any, is needed to capture the cost savings that generics can offer.
“The one reason that a lot of plans put it on special authorization is because of this explosive growth for using it for weight loss, and that's an interesting dynamic because in Canada, weight loss drugs have historically been considered optional benefits,” says Stevenson. “And so one of the dilemmas is for people that then use Ozempic off-label for weight loss, they're getting coverage, but if you have a plan where Ozempic isn’t covered for weight loss and you need approval, you might not get access to it.”
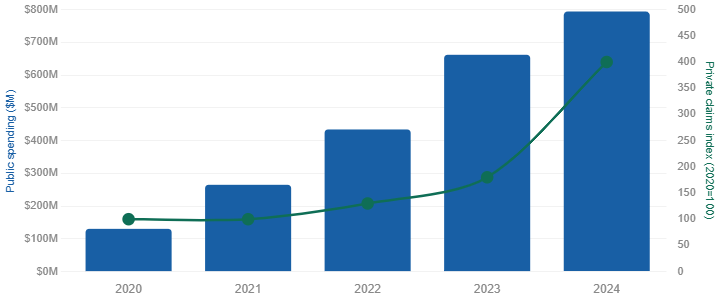
Blue: Public-plan spending on Ozempic. Green: Private weight-management drug claims. Sources: CIHI public drug spending data; TELUS Health Drug Data Trends report; Globe and Mail / IQVIA Canada. Private claims index (right axis) is estimated from TELUS Health reporting that weight management spending more than quadrupled since 2021 and doubled in 2024 following the launch of Wegovy.
The broader benefits picture
Total claims paid out by Canadian insurers for weight-loss drugs spiked to $77 million in 2024, up from nearly $38 million the year prior, reported the Globe and Mail. However, group benefits and health policy consultant Chris Bonnett, Principal of H3 Consulting, offers a broader lens on the financial stakes. He says that focusing narrowly on price misses the bigger clinical picture: “The biggest mistake all drug plans make is weighing coverage based on price, cost, or budget impact without understanding the clinical effects and overall value to patients, other payers, and society at large,” says Bonnett.
He points to the complexity of comorbidities as a key consideration: there are 13 cancers associated with obesity and overweight, and between 20 and 30 per cent of cancer patients are also diagnosed with diabetes, heart disease, depression, or anxiety. Treating these conditions in isolation, he says, is a strategic error.
Bonnett believes that national pharmacare is unlikely to change this equation much in the near term. The federal program covers a limited formulary of older diabetes drugs in only four jurisdictions – representing just 18 per cent of Canada's population – and GLP-1 drugs remain ineligible, so private drug plans will continue to play a critical role in patient access, he says.
What HR leaders should do now
Stevenson frames the generic GLP-1 question as part of a much larger structural shift in drug plan management – one that demands more attention than it typically receives.
“Drug plans have gotten so complicated, with the huge number of new drugs coming to market,” she says. “We're just in an area where I would characterize it as no longer a drug trend – it's a real structural shift in drug plans that requires more attention and some focus.”
For plan sponsors who have Ozempic on an open formulary with generic substitution already in place, the transition to lower-cost alternatives may largely take care of itself. For those with special authorization requirements, a deliberate plan design review is needed, according to Stevenson.
In addition, new, potentially higher-cost GLP-1 therapies continue to emerge, so the question of value – weighing clinical benefit against cost – becomes even more urgent, says Bonnett. “Plan sponsors and insurers will need to monitor GLP-1 spending and should ensure that patients are also following diet and exercise regimens that together help create and sustain diabetes control, weight loss, and better overall health."
Canada may have led the G7 in approving generic semaglutide, but for HR and benefits leaders, the real work of managing these drugs thoughtfully is only just beginning.


